 |  |
|
|---|---|---|
| Gastric Bypass Surgery | Duodenal Switch | |
| Method of Weight Loss | Restrictive & Malabsorptive | Restrictive & Malabsorptive |
| Duration of Procedure | 2 Hour | 4 Hour |
| Length of Hospital Stay | 2-3 Nights | 2-3 Nights |
| Estimated Weight Loss | 70% of Excess Weight | 65-90% of Excess Weight |
| Weight Loss at 1 Year | 60-80% | 70% |
| Comorbidities | Higher Resolved | Significant Resolved Rates |
| Hypertension Resolved | 69% | 43% |
| Diabetes Resolved | 83% | 92-100% |
| Migrations Resolved | 57% | Major Improvements |
| GERD Resolved | 80% | 49% |
| Mortality | 0.3% | |
| Asthma | 80% | 90% |
| Sleep Apnea | 98% | 85% |
| Depression | Most Resolved | 57% |
| Quality of Life Improved | 95% | 95% |
| Common Complications | Anastomotic Leaks 5% | N/A |
| Common Side Effects | Nausea, Digestive Issues | GERD, Gallstone, Bowel Movement |
| Recovery | 2 to 4 Weeks | 2 to 4 Weeks |
| Cost: Self-Pay Average | $25,000 | $30,000 |
| Cost w/ Renew Bariatrics | $6,299 | Not Offered |
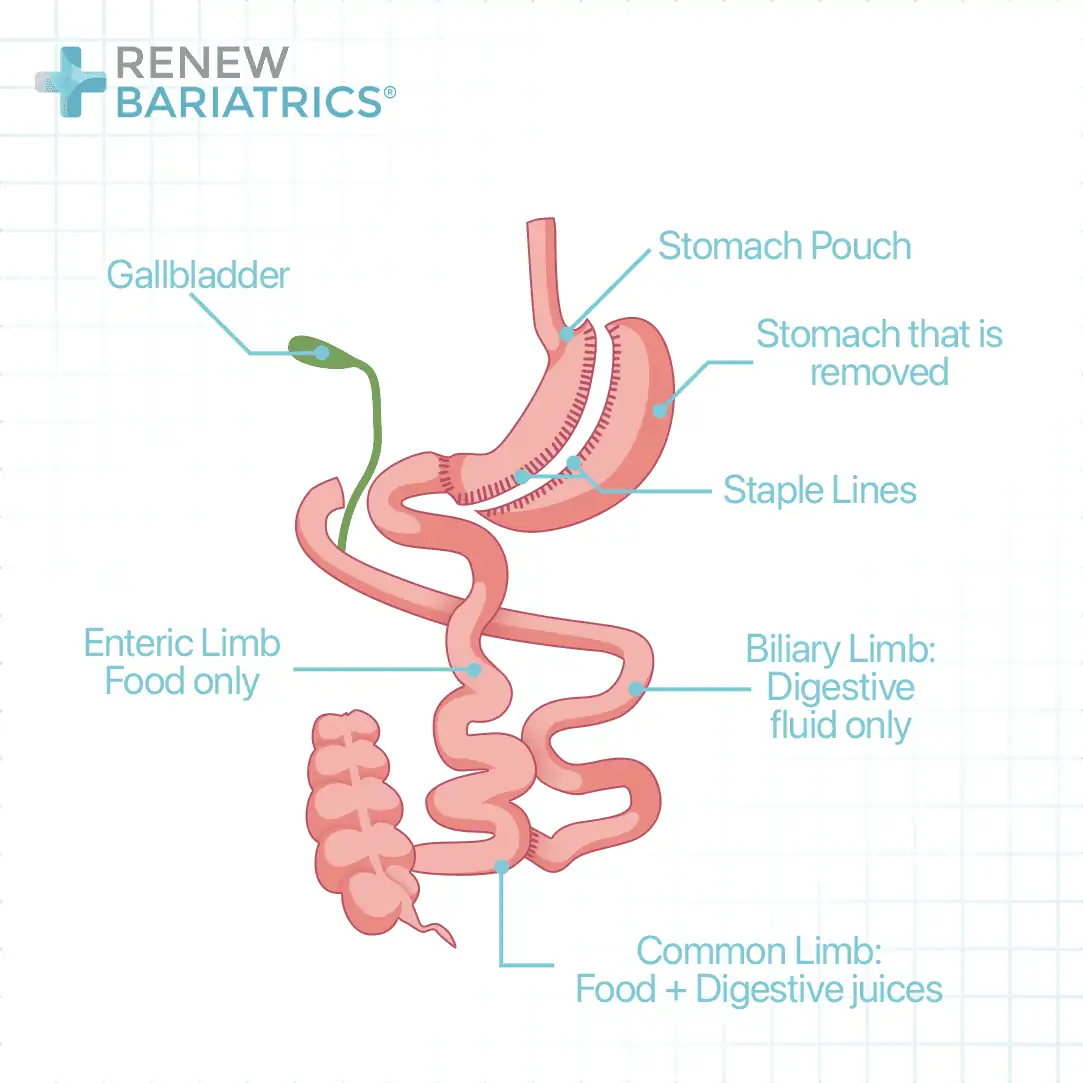
In a duodenal switch, the capacity of the stomach is also reduced by a gastric sleeve surgery. The intestine is then refashioned in such a way as to prevent the bile and pancreatic enzymes from coming in contact with the food until about 50cm from the junction between the small and the large intestine.
This is achieved by dividing the duodenum (1st part of the small intestine). The lower end of the gap is closed and turned to a blind end. The small intestine is again divided at the about 250cm from where it joined the large intestine. The upper end is joined to the small intestine at about 50cm from where it entered the large intestine. The lower end is joined to the upper end of the first point of division. With this arrangement, absorption will not take place in a relatively longer part of the intestine than what obtains in gastric bypass.
